Aprotinin use and monitoring
Aprotinin is indicated for prophylactic use to reduce blood loss and blood transfusion in adult patients at high risk of major blood loss undergoing isolated CABG. (i.e. coronary artery bypass graft surgery that is not combined with other cardiovascular surgery).1 Aprotinin should only be used after careful consideration of the benefits and risks, and the consideration that alternative treatments are available.1
Aprotinin should not be used when isolated CABG surgery is combined with another cardiovascular surgery, because the benefit–risk balance of aprotinin in other cardiovascular procedures has not been established.1Aprotinin should only be used after careful consideration of the benefits and risks, and the consideration that alternative treatments are available.1
Hypersensitivity to aprotinin: Allergic/anaphylactic reactions are rare in patients with no prior exposure to aprotinin. Administration of aprotinin to patients with a suspected previous exposure including in fibrin sealant products during the last 12 months is contraindicated. In the case of re-exposure, the incidence of allergic/anaphylactic reaction is 5.0% in patients with re-exposure within six months, and 0.9% in cases with re-exposure more than six months after initial administration. A retrospective review suggests that the incidence of severe anaphylactic reactions to aprotinin may further increase when patients are re-exposed more than twice within 6 months. Even when a second exposure to aprotinin has been tolerated without symptoms, a subsequent administration may result in severe allergic reactions or anaphylactic shock with, in very rare cases, fatal outcome.1
Please find the summary of product characteristics here for more information.
Monitoring of anticoagulation during cardiopulmonary bypass
Aprotinin is not a heparin-sparing agent and it is important that adequate anticoagulation with heparin is maintained during aprotinin therapy.1
The partial thromboplastin time (PTT) and activated partial thromboplastin time (APTT) become immeasurable with high doses of heparin. Therefore APTT and PTT should not be used to monitor anticoagulation with heparin in patients undergoing CABG. One of the following methods are recommended to maintain adequate anticoagulation:1
- Individualised heparin and protamine management
- Or, if unavailable, regular activated clotting time (ACT) tests, with heparin doses given accordingly
- If ACT is used, a minimal celite-ACT of 750 seconds or kaolin-ACT of 480 seconds, independant of the effects of haemodilution and hypothermia, is recommended
Before prescribing aprotinin, please see SmPC for further information on monitoring and anticoagulation during CABG.
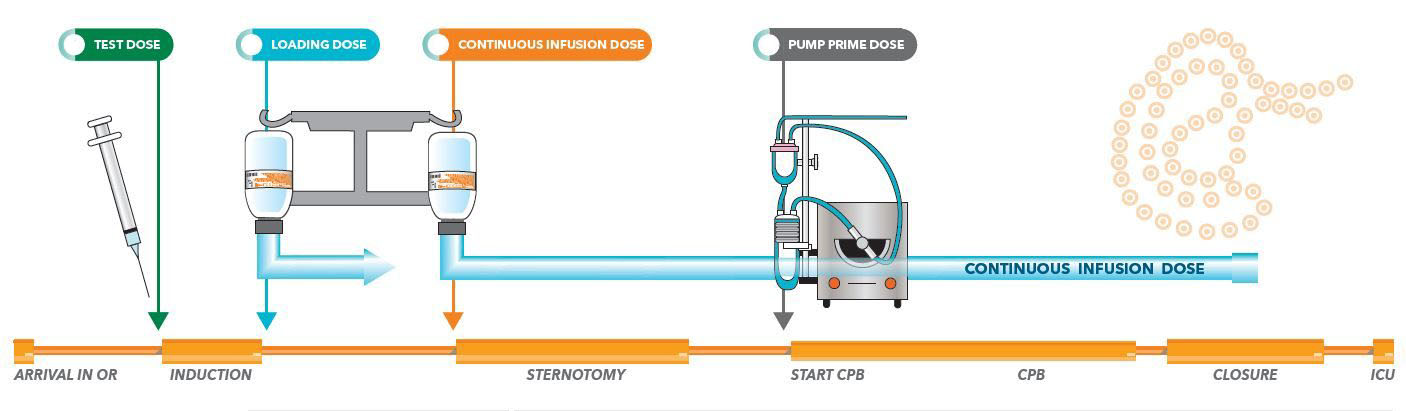
| DOSAGE | ADMINISTRATION | |
| TEST DOSE | 10,000 KIU (1ml) | The test dose should be administered intravenously to all patients at least 10 minutes prior to loading dose |
| LOADING DOSE | 1 – 2 million KIU
(2-4 vials of 50 ml) |
A loading dose of 1 – 2 million KIU is administered as a slow intravenous injection or infusion over 20 – 30 minutes after induction of anaesthesia and prior to sternotomy. A further 1 – 2 million KIU should be added to the pump prime of the heart-lung machine. |
| CONTINOUS INFUSION DURING SURGERY | 250,000 – 500,000 KIU per hour
(0.5 to 1 vial per hour) |
After the initial bolus infusion (loading dose) until the end of the operation |
| PUMP PRIME DOSE | 1 – 2 million KIU
(2 – 4 vials of 50ml) |
TO BE ADDED TO THE PUMP PRIME OF THE HEART-LUNG MACHINE To avoid physical incompatibility of aprotinin and heparin when adding to the pump prime solution, each agent must be added during recirculation of the pump prime to assure adequate dilution prior to admixture with the other component |
One vial of 50ml of aprotinin contains 500,000 KIU
Aprotinin 10,000 KIU/ml Injection BP. Note: It is important that adequate anticoagulation with heparin be maintained during aprotinin therapy. Elevations in the partial thromboplastin time (PTT) and Celite-Activated Clotting Time (Celite ACT) are expected in aprotinin-treated patients during surgery, and in the hours after surgery.
References
- Aprotinin 10,000 KIU/ml Injection BP Summary of Product Characteristics. Available from: https://www.medicines.org.uk/emc/product/2472/smpc.
